Athletic Groin Pain: Part 1
Athletic Groin Pain
Part 1: Anatomy and Pathology of Potential Injuries
Groin pain is a common injury among athletes, especially multidirectional athletes. The most common sports for groin pain are hockey and soccer, but any sport that requires frequent changes of direction will increase your risk, especially in high level males. In this blog post, we will discuss multiple different potential causes of athletic groin pain.
When diagnosing groin pain I like to first think about breaking the cause of pain into intra-articular vs. extra-articular. Intra-articular structures are those that are part of the hip joint itself. Extra-articular structures are those that sit outside the joint but that still play an important role in the function of the joint.
- Intra-articular pathology (for the purposes of this blog) include:
- Osteoarthritis
- Femoroacetabular Impingement
- Labral Tears
- Ligamentum Teres Tears
- Extra-articular pathology (for the purposes of this blog) include:
- Athletic Pubalgia/Sports Hernia
- Inguinal Related
- Pubic Related
- Adductor Related
- Hip Flexor Related
- Acute Adductor Injuries/Strain

Why are multidirectional athletes more likely to get groin pain?
- Our hip is a ball-in-socket joint….a very stable ball-in-socket joint. There is a deep articulation of the femur within the acetabulum of the hip. This articulation is deepened by a ring of cartilage surrounding the hip socket called the labrum. As the hip joint moves around within the joint, our “femoral neck” is expected to abut against the acetabulum/labrum. This over time can lead to pain.
- Their hips also go through a lot of high force rotational activity that is easy to miss in a training program, or their only training is their sport which can lead to overuse injury.
We have adopted a catch all term for pain when the femur abuts against the acetabulum called “Femoroacetabular Impingement” (FAI) and similar to many other “medical syndromes” it is more based on a cluster of symptoms rather than one stand alone finding.
So what do medical professionals look for in order to diagnose someone with FAI?
- Clinical Signs and Symptoms
- Hip pain with hip movements: If the symptoms are coming from the femur and acetabulum coming together, a clinician can in theory, move your hip in a way to approximate those two structures, and add a little bit of extra pressure to attempt to reproduce symptoms indicating that the pressure of the femoral neck abutting against the acetabular rim is a contributing factor to pain.
- Healthcare providers are also looking for symptoms such as: pain during activity, stiffness after activity and pain after activity as pain at rest is a rare finding with FAI.
- Imaging Findings
- There are 2 types of “morphology” that can be detected on imaging: Cam Morphology and Pincer Morphology.
- Pincer Morphology:
- This is more common in females and is an excessively deep hip socket that causes the femur to make contact with the acetabulum earlier than normal. The contact itself is not the issue. Everyone makes contact with their acetabulum many times daily, however, all of our body tissues do have a limit so if you are making more contact and your muscles have less time to dissipate force before contact occurs due to excessive coverage it may be more likely to become symptomatic than someone with a little bit less coverage of their femoral head.
- Impingement with a Pincer morphology is normally a little bit more anterior and will be reproduced with hip flexion combined with adduction and internal rotation called the “FADIR Test”
- Cam Morphology
- Cam morphology is more common in males and is thought in many cases thought to be a bony adaptation to high level sports.
- Wolf’s law indicates that bones will adapt to the stress and demand placed on them. In very high level youth sports, young, developing children put their body through high stress repetitive activities. In the case of soccer and hockey, this involves an extended, abducted and externally rotated lower extremity. At the higher levels, these children are faster and stronger which creates a higher level of force. During repetitive kicking and skating activities, the posterior femoral neck will actually adapt to the extra stress by increasing in size. This increase in size is great for the bone itself, but can create an issue down the road by again abutting against the acetabulum earlier making it more likely to overload the approximating tissues (bone/labrum) and create pain.
- This bony adaptation will often limit the ability of one’s knee to fall outward and can be assessed using a test called the “FABER Distance” test where the knee is allowed to fall outward and the distance from the knee to the table is measured. If there is a difference of > 3.7 cm between symptomatic and non-symptomatic sides there is a 75-80% chance a Cam morphology is present.
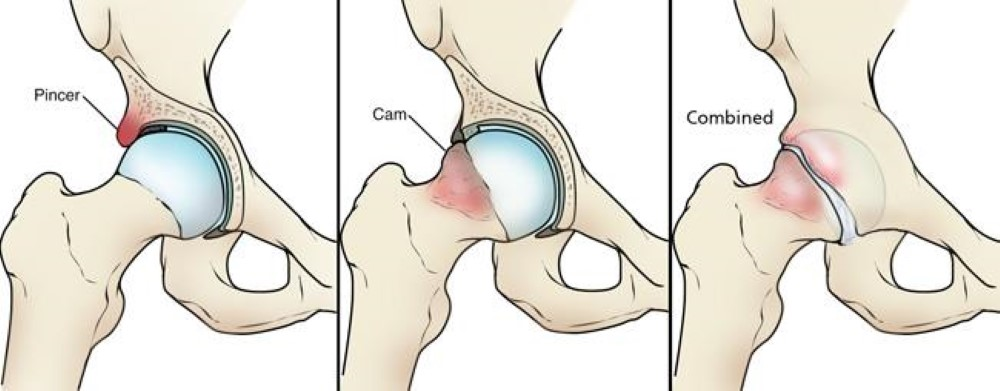
https://orthoinfo.aaos.org/en/diseases--conditions/femoroacetabular-impingement/
Ok, so how is it treated?
- Treatment of FAI is going to depend on some different factors, but one of the most important will be exacerbating and relieving positions.
- We discussed 2 types of FAI above (Cam and Pincer morphology), however they are often present in conjunction with each other, furthermore, just because there is presence of FAI on imaging does not mean that a person’s pain is from the morphology itself, so that is where the clinical examination comes into play. The hip should be placed into positions where impingement is expected to occur. The location of pain reproduction will help guide decision making for choice of intervention.
- Ultimately it will come down to modification of activity in the short term with rehab exercises focused on targeting mobility, strength, and movement strategy impairments that when deficient may increase the risk of creating a symptomatic impingement. This will vary based on the type of impingement, and the athlete’s sport of choice.
- Much of the treatment will be centered around decreasing the intensity of the femur abutting against the acetabulum.
- This will be performed through improving mobility of structures surrounding the hip joint (ankle, knee, low back, thoracic spine, and sometimes even the neck and shoulders depending on the sport).
- It is also important to have strong musculature to help control the speed at which the femur abuts the acetabulum. Strong hip, core, and thigh musculature will help to dissipate the high levels of forces that the hip must endure during multidirectional sports.
- Surgical options are not great at this time. Hopefully in the future techniques continue to develop but at this time the first course of action will normally be a bout of physical therapy followed by a gradual resumption of desired activities to allow the tissue to readapt to the high degree of stress that it will need to endure with sporting activity. Even those that have a “good” outcome after surgery commonly see a drop off in athletic performance or are unable to return to sport at their previous level.
- There are also some concomitant pathologies that come into the decision making process.
- Microinstability:
- The classic patient with microinstability will be:
- Young female adult who participates in sporting activity that requires a high level of flexibility and excessive ROM.
- They may feel groin or anterolateral hip pain and apprehension or a sensation of instability.
- This patient may benefit from a program focusing on strengthening of their gluteal musculature and a small group of muscles that as a group are called “external rotators” which serve to stabilize the femoral head within the acetabulum.
- Subspine Impingement:
- This is not a very common pathology, but may be present in those who have had a previous AIIS avulsion.
- AIIS avulsions can happen during sporting activity and is more common in adolescent and young adult males.
- Acetabular Labral Pathology:
- Labral tears will present similarly to FAI but those with labral tears are more likely to have pain at night.
- Labral tears are more likely to present with symptomatic clicking or catching of the hip joint.
- Labral tears are very common in sports that involve a high degree of impingement, in fact, as many as 66% of asymptomatic individuals will present with a labral tear on MRI.
We will now shift gears and discuss Athletic Pubalgia which is another catch all term for groin pain that is of muscular origin as opposed to FAI and other pathologies discussed above that are from cartilage or other non-muscular tissues of the hip joint. You may also hear the term “sports hernia” which is another general term for pain caused by some type of overuse injury to the muscles of the lower abdominal / anterior hip and groin region. It is very common to feel no pain at rest but with physical activity you will likely have progressive worsening of pain that will subside within a few hours to a day or so after stopping the activity.
When treating athletic pubalgia, it may be beneficial to differentiate what specific musculature is involved. In order to better accomplish this, your rehab provider should do their best to “subtype” the cause of the pain to help guide treatment.
The 4 subtypes of athletic pubalgia are:
- Adductor related
- Hip flexor related
- Inguinal related
- Pubic related.
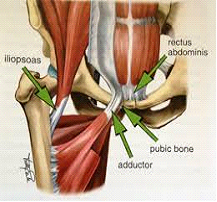
http://stoverpt.com/uploads/3/4/8/2/34823947/7660189_orig.png
{kind=link}
Diagnosing each subtype involves strength testing hip and core musculature to determine which seems to be the most symptom producing. From that point, rehab can begin to gradually stress the weakened musculature and work on improving impaired ROM that may increase risk of injury. During rehab it may be important to alter your physical activity, training, or competition participation.
Every sport has their repetitive movements that lead to chronic injuries. In high level, multidirectional athletes, the groin and lower core musculature undergo a lot of stress and if not properly prepared for activity can begin to breakdown and create pain. Soccer players place a very high demand on their hip flexors, groin, and lower core as they extend and externally rotate their hip, then swing it through with maximal force to kick a soccer ball. Hockey players are constantly pushing their hips into forceful extension and abduction to accelerate on the ice adding an eccentric strain to the adductor and hip flexor musculature. When this is coupled with the fact that they are in a flexed position when skating creating an adaptive shortening of their hip flexor musculature overtime, if they are not diligent about a stretching and mobility program, the forceful hip extension required for sport begins to create strain on the hip flexor musculature earlier in the range of motion and may increase their chance of developing groin/anterior hip pain.
We will discuss a little more about the theory of and potential training modifications to improve an athlete’s tolerance to these activities and decrease their risk of developing athletic pubalgia / a sports hernia in part 2 of this blog post.
Athletic pubalgia is a chronic issue, but acute strains can occur to the adductor region. Diagnosis of an adductor strain involves strength testing the adductor musculature to assess for pain reproduction, pain with stretching of the musculature, and a mechanism of injury. After an acute groin injury it is important to keep moving in a way that is relatively pain free, but it is not wise to aggressively stretch or strengthen the damaged tissue for at least the first 2-3 days and you should consult with a rehab professional to help guide the progression back to sport.
When you are injured, it is important to seek the care of a physical therapist to guide you through the rehab process. However, if you play a multidirectional sport, it may be important to make some adjustments to your training program in order to best prepare your body for the demands of multidirectional and rotational sports.
Learn more about prevention of athletic groin pain in part 2 of this blog post series.
Your blog is really good. This information is really useful for those who have searched for this and you have great knowledge about this. I’m really impressed with your post. hip pain clinic Scottsdale AZ
ReplyDeleteI read the above article and got some knowledge from your article which is about Anatomy and Pathology of Potential Injuries It's actually great and useful data for us. Thanks for sharing it. Best surgeon in Bakersfield CA
ReplyDeleteI am very much obliged to you for sharing this necessary knowledge. This information Best surgeon in Bakersfield CA is very helpful for everyone. So please always share this kind of information. Thanks once again for sharing it.
ReplyDeleteThanks for your post. It's very helpful post for us. You can also visit Auto Accident Injury Treatment Mesa Az for more Victor Steel related information. I would like to thanks for sharing this article here.
ReplyDeleteI am very thankful to for the post you have shared here about Athletic Injury is really helpful for me about Athletic Injury Management in Calgary Thank you for sharing that. Keep up the good work.
ReplyDeleteI generally want quality content and I found that in your post. The information you have shared about Chiropractic Therapy Panorama Hills is beneficial and significant for us. Keep sharing these kinds of articles here. Thank you.
ReplyDeleteThe information in the post you posted here is useful because it contains some of the best information available. Thanks for sharing about massage therapy airdrie. Keep up the good work.
ReplyDeleteThis comment has been removed by the author.
ReplyDeleteI always check this type of advisory post and I found your article which is related to my interest.plantar fasciitis treatment This is a great way to increase knowledge for us. Thanks for sharing an article like this.
ReplyDeleteYou've done a great job with your ideas. Your essay has a wealth of useful information about Bryan Hospital. It is, without a doubt, a vital article for us.
ReplyDeleteA very delightful article that you have shared here about Physical Therapy Findlay. Your blog is a valuable and engaging article for us, and also I will share it with my companions who need this info. Thankful to you for sharing an article like this.
ReplyDeleteClearly, It is an engaging blog for us that you have provided here about Pain Relief Gel This is a great resource to enhance our knowledge about it. Thank you.
ReplyDeleteYou have referenced here incredible data here. I might want to say this is a very much informed article and furthermore gainful article for us. Continue to share this sort of articles, Thank you.Shop Knee Support Sleeve Online
ReplyDeleteThis article you've just presented is appealing. I'd like to learn more about these types of blogs. Thank you so much for sharing this blog. psychiatrist san antonio tx
ReplyDeleteYou have done a good job by publishing this article about Bone density test cost I appreciate your efforts which you have put into this article, It is a beneficial article for us. Thanks for sharing such informative thoughts.
ReplyDeleteSuccess counseling helps individuals identify and achieve their goals. Sexual Trauma Treatment
ReplyDeleteThank you for this insightful article on athletic hip pain. It's encouraging to learn about the common causes and risk factors associated with hip pain in athletes. Understanding these factors is crucial for effective prevention and management. For those interested in exploring additional recovery options, Vita Bella offers a range of products and therapies designed to enhance healing and restore vitality.
ReplyDeleteGreat breakdown of athletic hip pain! The distinctions you made really helped me understand different causes. For anyone also dealing with knee issues, this Gae Knee Treatment tool could be helpful. Looking forward to Part 2!
ReplyDelete