Concussion Evaluation and Treatment
Subjective:
Concussion Symptom Checklist
Please report your symptoms on the following scale: 0 = no symptoms; 6 = severe symptoms.
If you are being seen post-injury please fill out based on how you feel at this moment in time.
If you are being seen for baseline screening, please fill out based on how you typically feel.
Adapted from SCAT 5
Sport concussion assessment tool - 5th editionBritish Journal of Sports Medicine 2017;51:851-858.
Buffalo Concussion Treadmill Test
Protocol
Preparation Equipment Requirements
Preparation Equipment Requirements
- Treadmill with capacity to reach 15 degrees of elevation Note: Test can be adapted for treadmills which can reach a minimum of 12 degrees elevation
- Heart rate monitor (Polar brand recommended)
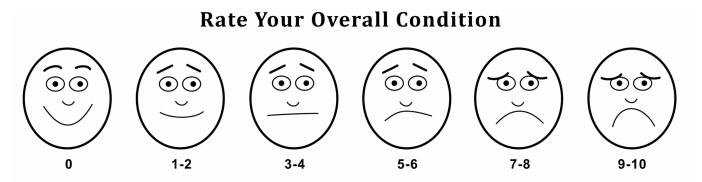
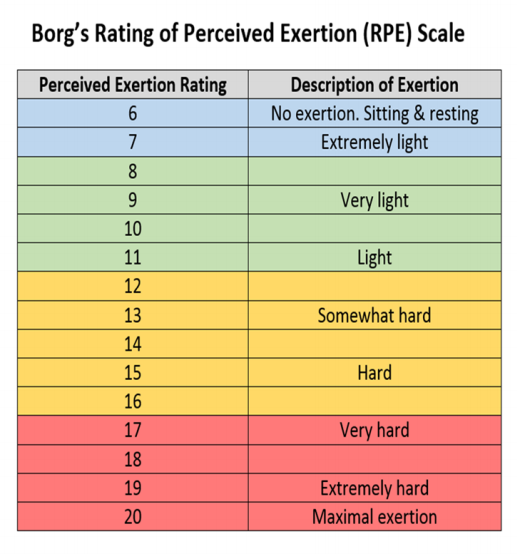
- Borg RPE Scale (Rating of Perceived Exertion) and Concussion Symptom Severity Scale (Likert scale) – See form attached
- Test Results form for monitoring heart rate, changes in RPE and symptoms, and relevant observations – See form attached
- Chair, water and towel for participant recovery after exercise
Setup
- Attach heart rate monitoring device according to manufacturer’s instructions
- Post RPE and Symptom scales within comfortable viewing distance of participant while on treadmill (it is suggested that participant should not have to turn head to view scales)
Test Protocol
Starting the Test
- Inform participant about test procedures and what to expect during the BCTT.
- Explain and demonstrate the RPE and Likert scales and obtain resting scores. Remind participant that he/she will be asked to rate exertion and symptom severity at each minute during exercise. The RPE scale is a measure of perceived physical activity, and can be explained to participants as a measure of “how hard you feel like your body is working”. The scale’s numbers (6-20) and descriptors should be pointed out. The Likert symptom scale is a measure of symptom severity (“how good/bad your symptoms are making you feel right now”), and should be distinguished as being distinct from RPE. The scale’s numbers (1-10) and pictures (expressions of physical pain) should be pointed out.
- Patient should begin by standing on the ends of the treadmill while the treadmill is turned on.
- The experimenter should set treadmill at a speed of 3.6mph for patients over 5’5”, and 3.2mph for those 5’5” and under.
- Starting incline is 0 degrees. Speed can be adjusted depending on athletic status or overall comfort of treadmill speed – patients should be moving at a brisk walking pace.
- After one minute at this pace, treadmill incline is increased to 1 degree. Participant is asked to rate RPE and symptom severity. Subjective scores and heart rate (bpm) are recorded.
- This procedure is repeated each minute, with ratings and heart rate being recorded, and treadmill increasing in incline at a rate of 1 degree/minute.
- Changes to Likert rating should be specifically clarified/noted (for example, if the rating moves from 2 to 3, it should be clarified if this reflects the addition of a new symptom, increased severity of an existing symptom, etc.).
- Experimenter should also record general observations as the test progresses.
- Once treadmill reaches maximum incline (15 degrees or 12 degrees in modified test), speed is increased by 0.4mph each minute in lieu of increased incline.
- Once test is terminated (see below), speed is reduced to 2.5mph and incline reduced safety back to 0 for a 2 minute cool-down (if participant is safe to continue).
- During this time, Likert ratings should continue to be reported each minute.
- Test continues until
- Maximum exertion (RPE score of 19.5) is reported or
- Test is terminated by experimenter due to a symptom exacerbation that causes significant increase in pain or symptom severity (an increase of more than 3 points on the Likert scale from resting score, addition of several new symptoms, or marked increase in severity of symptoms resulting in difficulty continuing test)
- Experimenter notes a rapid progression of complaints (ex. headache to searing focal pain) between symptom reports, patient appears faint or unsteady, or determines that continuing the test constitutes significant health risk for the participant, or
- Patient reports an inability to continue the test safely
Vestibular Ocular Motor Screening (VOMS):
Instructions:
Interpretation
Interpretation
- This test is designed for use with subjects ages 9-40. When used with patients outside this age range, interpretation may vary. Abnormal findings or provocation of symptoms with any test may indicate dysfunction – and should trigger a referral to the appropriate health care professional for more detailed assessment and management.
Equipment
- Tape measure (cm)
- Metronome
- Target w/ 14 point font print
Baseline Symptoms
- Record: Headache, Dizziness, Nausea & Fogginess on 0-10 scale prior to beginning screening
Smooth Pursuits
- Test the ability to follow a slowly moving target.
- The patient and the examiner are seated. The examiner holds a fingertip at a distance of 3 ft. from the patient. The patient is instructed to maintain focus on the target as the examiner moves the target smoothly in the horizontal direction 1.5 ft. to the right and 1.5 ft. to the left of midline.
- One repetition is complete when the target moves back and forth to the starting position, and 2 repetitions are performed.
- The target should be moved at a rate requiring approximately 2 seconds to go fully from left to right and 2 seconds to go fully from right to left. The test is repeated with the examiner moving the target smoothly and slowly in the vertical direction 1.5 ft. above and 1.5 ft. below midline for 2 complete repetitions up and down. Again, the target should be moved at a rate requiring approximately 2 seconds to move the eyes fully upward and 2 seconds to move fully downward.
- Record: Headache, Dizziness, Nausea & Fogginess ratings after the test.
Saccades
- Test the ability of the eyes to move quickly between targets. The patient and the examiner are seated.
- Horizontal Saccades
- The examiner holds two single points (fingertips) horizontally at a distance of 3 ft. from the patient, and 1.5 ft. to the right and 1.5 ft. to the left of midline so that the patient must gaze 30 degrees to left and 30 degrees to the right. Instruct the patient to move their eyes as quickly as possible from point to point.
- One repetition is complete when the eyes move back and forth to the starting position, and 10 repetitions are performed.
- Record: Headache, Dizziness, Nausea & Fogginess ratings after the test.
- Vertical Saccades
- Repeat the test with 2 points held vertically at a distance of 3 ft. from the patient, and 1.5 feet above and 1.5 feet below midline so that the patient must gaze 30 degrees upward and 30 degrees downward. Instruct the patient to move their eyes as quickly as possible from point to point.
- One repetition is complete when the eyes move up and down to the starting position, and 10 repetitions are performed.
- Record: Headache, Dizziness, Nausea & Fogginess ratings after the test.
- Convergence
- Measure the ability to view a near target without double vision.
- The patient is seated and wearing corrective lenses (if needed).
- The examiner is seated front of the patient and observes their eye movement during this test. The patient focuses on a small target (approximately 14 point font size) at arm’s length and slowly brings it toward the tip of their nose.
- The patient is instructed to stop moving the target when they see two distinct images or when the examiner observes an outward deviation of one eye. Blurring of the image is ignored.
- The distance in cm. between target and the tip of nose is measured and recorded. This is repeated a total of 3 times with measures recorded each time.
- Record: Headache, Dizziness, Nausea & Fogginess ratings after the test. Abnormal: Near Point of convergence ≥ 6 cm from the tip of the nose.
- Vestibular-Ocular Reflex (VOR) Test
- Assess the ability to stabilize vision as the head moves. The patient and the examiner are seated. The examiner holds a target of approximately 14 point font size in front of the patient in midline at a distance of 3 ft.
- Horizontal VOR Test
- The patient is asked to rotate their head horizontally while maintaining focus on the target. The head is moved at an amplitude of 20 degrees to each side and a metronome is used to ensure the speed of rotation is maintained at 180 beats/minute (one beat in each direction).
- One repetition is complete when the head moves back and forth to the starting position, and 10 repetitions are performed.
- Record: Headache, Dizziness, Nausea and Fogginess ratings 10 sec after the test is completed.
- Vertical VOR Test
- The test is repeated with the patient moving their head vertically. The head is moved in an amplitude of 20 degrees up and 20 degrees down and a metronome is used to ensure the speed of movement is maintained at 180 beats/minute (one beat in each direction).
- One repetition is complete when the head moves up and down to the starting position, and 10 repetitions are performed.
- Record: Headache, Dizziness, Nausea and Fogginess ratings after the test.
- Visual Motion Sensitivity (VMS) Test
- Test visual motion sensitivity and the ability to inhibit vestibular-induced eye movements using vision.
- The patient stands with feet shoulder width apart, facing a busy area of the clinic.
- The examiner stands next to and slightly behind the patient, so that the patient is guarded but the movement can be performed freely.
- The patient holds arm outstretched and focuses on their thumb. Maintaining focus on their thumb, the patient rotates, together as a unit, their head, eyes and trunk at an amplitude of 80 degrees to the right and 80 degrees to the left. A metronome is used to ensure the speed of rotation is maintained at 50 beats/min (one beat in each direction).
- One repetition is complete when the trunk rotates back and forth to the starting position, and 5 repetitions are performed.
- Record: Headache, Dizziness, Nausea & Fogginess ratings after the test.
Cervical Spine Assessment
Balance Error Scoring System (BESS)
Testing Procedure:
- If test is being performed in clinic, have the patient remove shoes, socks may be worn if desired.
- Patient is instructed to perform each of the test conditions with hands on iliac crests and eyes closed.
- Each condition is performed for 20 seconds
- Errors are recorded for each position: Maximum 10 errors per position.
- If the patient commits multiple errors simultaneously only one error is recorded
- If the patient is unable to maintain test position for 5 seconds the patient is given a maximum error score of 10 for that test condition.
- Double leg stance is performed with feet together (touching).
- Single leg stance is performed on non-dominant foot
- Tandem stance is performed with non-dominant foot in back
- Dominant foot is described as their preferred kicking foot.

Postural Orthostatic Tachycardia Syndrome:
* If yes, borderline, or if there is any suspicion of abnormality refer back to the physician.
Additional Ocular Assessment:
Acuity: Snellen Chart
- Vision 20/25 or better: (Y/N): ______
- If no, refer to optometrist
- If you have a 20/20 Snellen Chart, place patient 20 feet away and assess vision
- Assess binocular and monocular vision
- If they can’t see, we can’t help them, be sure to refer
Visual Field:
- Test 1: Gross Deficit
- Therapist seated across from patient and asks if any parts of the therapists face are missing which indicates a gross visual field deficit
- Test 2: Quadrants
- Therapist seated across from patient, patient closes one eye and therapist closes the mirror of that eye.
- Patient is instructed to keep their eyes on the therapist’s nose
- Therapist holds the number 1 or 2 in each quadrant (UR, UL, LR, LL) mid-way between therapist and patient. If the patient is unable to identify the number, they have a visual field loss in that quadrant; repeat w/ other eye.
- **Do not hold finger close to end range as everyone’s visual field will be a little different. This is a screen for RED FLAG visual field loss, do not try to beat the patient.
- Test 3: Quadrants (end range)
- Same starting position as above; Patient is instructed to keep their eyes on the therapist’s nose during the test.
- Therapist brings finger from end range of each quadrant toward the middle of the theoretical box over the patient’s open eye and patient tells therapist when they are able to see the finger.
- Once again, this is a screen and there will be minor differences. We are looking for gross visual field deficits.
- If any visual field testing is positive or suspicious, refer.
- Screening for dysfunction of ocular muscles and potentially cranial nerve involvement
- Patient is seated appropriate distance from eye chart and is asked to read the lowest line that they are able.
- Therapist holds the patient’s head and rapidly shakes head side to side at a rate of 2 Hz (240 bpm) and patient is again asked to read the lowest line possible
- A loss of > 3 lines is positive
- Dorsal Visual Stream: Fast (preconscious)
- The “Where is it” pathway
- Peripheral awareness, motion detection, location of objects
- Transfers from occipital lobe to parietal lobe
- Ventral Visual Stream: Slow
- The “What is it” pathway
- Identification and classification of objects, color and detail
- Tightly focused w/ hyper detail
- Transfers from the occipital lobe to the temporal lobe
- If the ventral stream is hyper-active, everywhere they go, they will be focusing on the little details of everything and it can potentially cause headache or other symptoms.
- Can assess for benefit with binasal occlusion
- Fold a piece of paper into a triangle (~ 30 degree angle) and slide from superior to inferior into patients field of vision.
- The patient lets you know when the paper becomes “disruptive”
- Mark on the paper where the disruption to visual field occurs and place a piece of scotch tape on the patient’s glasses (or on a pair of non-prescription glasses if patient does not have glasses).
- This in theory will make it difficult and not desirable to focus on things and will hopefully downregulate the ventral stream.
- Accommodation vs. Convergence
- Have the patient look at a near target letter and a far target letter with 2 eyes, then with 1 eye, then the other eye.
- Greater difficulty with both eyes indicates a convergence issue as the eyes are unable to work together to focus on a target.
- Greater difficulty with one eye indicates an accommodative issue.
- The lens is under resting tension from the ciliary fibers and is in a flattened state which allows us to see farther away. The ciliary muscles contract and take slack off of the ciliary fibers allowing the lens to be in a more rounded state which allows us to see closer.
- Accommodative Spasm: Ciliary muscles are unable to relax and it is difficult to see objects farther away (especially when performing with 1 eye at a time)
- May present as difficulty with prolonged computer use or reading.
- Those with convergence dysfunction may see double while reading
- Those with accommodative dysfunction may had the words be more blurry than double.
- Difficulty looking from chalkboard to notes in school; or from traffic to dashboard while driving.
Ocular Treatment Strategies:
Smooth Pursuits:
Smooth Pursuits:
- Notes:
- Smooth pursuits are slow and are limited in speed to 30 deg/second. Going faster will not help smooth pursuits.
- Smooth pursuits are able to cancel VOR when tracking an object with head turn.
- If a patient is found to be teleporting within a certain range of movement, train the smooth pursuits in that range.
- Be sure to assess and train in all planes of motion: Horizontal, vertical, V, ^, H, I.
- Assess binocular and monocular and train both if both are impaired
- Marsden Ball Exercises
Saccades:
- Notes: Saccades are FAST: 400-700 deg/second
- 3 types:
- Voluntary saccades: Planned movement to a specific target.
- Reflexive: Unplanned movement to a target based on sudden appearance
- Wayne Saccadic Fixator
- Light Board - helps work on saccadic fixation and eye-hand coordination
- Anti-Saccades: Looking away from a target, assesses for the frontal lobes ability to suppress reflexive saccadic movement.
- Look at the box opposite of the box that lights up/look away from an object that comes into your line of sight. (failure to do so indicates poor frontal lobe or basal ganglia function and indicates referral)
- Hypermetric saccades are not consistent with concussion and indicate more serious pathology, likely cerebellar, and indicate referral.
- Abnormalities that can be treated in PT:
- Hypometric saccades - hypofunction
- Slowed Saccades - Caused by a subnormal peak in the activity of ocular motoneurons
- Symptomatic Saccades - gradually habituate and improve tolerance.
Accommodative Dysfunction:
- If they have difficulty focusing on near targets, their ciliary muscles are having a hard time getting the lens in the proper position to focus on near targets.
- Normal to have difficulty at age > 40. May indicate need for bifocals.
- Refer to neuro-optometrist for consideration of therapy vs. glasses
- Can practice near target-far target fixation with involved eye being sure to bring object into focus to try to get ciliary muscles to relax in the case of accommodative spasm.
Vergence Dysfunction:
- Will commonly have double vision or have to close 1 eye to see clearly.
- Convergence insufficuency: > 6cm
- Convergence Spasm: Eyes converge, but one or both have difficulty coming back out (diverging)
- Treatment:
- Pencil Push-ups
- Brock string
- V,X,A
- Ant on a string
- Head turned w/ string at 30 deg left and right
- Slight VOR x 1.
- Move beads and work in the trouble areas
- Near-Far Hart Chart
- Near-Far Hart Chart Decoding (Great for Kids)
- Dot Charts
- Playing catch
- Numbered Ball Tossing
- Other Considerations: If as they are performing their exercises, or during the assessment, they report that the “X” that they see is vertically stacked, they may need a prism lens and should be referred to neuro-optometry
VOR Dysfunction:
- Normal: 180 bpm, Athletes: 200 bpm.
- Treatment strategies:
- Position: Seated → Standing → FT → Tandem → SLS → Walking → Tandem walking
- Background: Plain → busy background → busy clinic → passenger in car
- Direction: Horizontal, vertical, V, ^
- Speed: Use metronome to increase and monitor progression
- Reading w/ VOR: Kids Book → More difficult book
- Can add recall for those that fall into the cognitive profile
- VOR with Ball Toss
Visual Motion Sensitivity:
- Visual related symptoms in response to a moving stimulus, especially encompassing the peripheral visual field.
- Unstable Ambient Vision (Magnocellular):
- Magnocellular pathway: Dominant in dorsal pathway
- Larger cell bodies, larger visual field, fast information; respond transiently to visual information, cannot perceive color
- Ambient environment
- Parvocellular: Dominant in ventral pathway
- Sustained information, color.
- Focal detail
- If there is a loss of the preconscious reflexes from the magnocellular pathway, everything becomes hyper-focused through sustained attention and focal blinding occurs.
- Can be overwhelming when the person gets into a busy environment (store, busy hallway, driving).
- Focal Blinding: Like driving through a snowstorm w/ high beams on.
- Patient has to really focus on point of interest with more effort causing exclusion of the periphery.
- More movement = more spatial disorientation
- Treatment:
- Binasal occlusion
- Helps to decrease strain on parvocellular pathway/ventral stream as it is unable to focus as hard and attempts to restore balance.
- Objects on the right can only be fixated on with the R eye, and vice versa, decreasing fixation strain and visual overstimulation
- Can also help w/ convergence excess and divergence deficits
- Optokinetics
- Act to desensitize
- Eye follows an object until it goes out of the field of vision then quickly moves to the point at which it saw the object at first
- Ex: Rotating umbrella
- Optokinetic video
- 1st 4 minutes easy, next 4 minutes medium, last 2 hard.
- Headaches in a raccoon eyes/lone ranger pattern, often with sustained reading
- Treatment: Eye recovery techniques
- Cup hands over eyes to remove light and open eyes and stare into palms in darkness for 1-2 minutes
Other Ocular Exercises:
- Headlamp: Good for cervical dysfunction as well
- Strap laser pointer to head → close eyes, rotate x10 → attempt to return to the starting point and see how close they are.
- http://eyecanlearn.com/
- Website for visual exercises for kids
- Any hand-eye coordination exercises
- Reflex ball
- Numbered ball
- Activities with VOR
- Stroop Chart
When to Refer with Ocular Issues:
- Hypermetric Saccades
- Improved Sx w/ binasal occlusion
- Lasik Surgery w/ monocular vision
- Lasik corrects one eye to see near and the other to see far. If they have a convergence deficit, their monocular vision that they have trained their brain to use will have to be broken, and once broken they will likely not be able to get it back, so be sure to discuss with neuro-optometrist and determine the best course of action and if convergence training will be best for the patient.
- Visual Field Loss
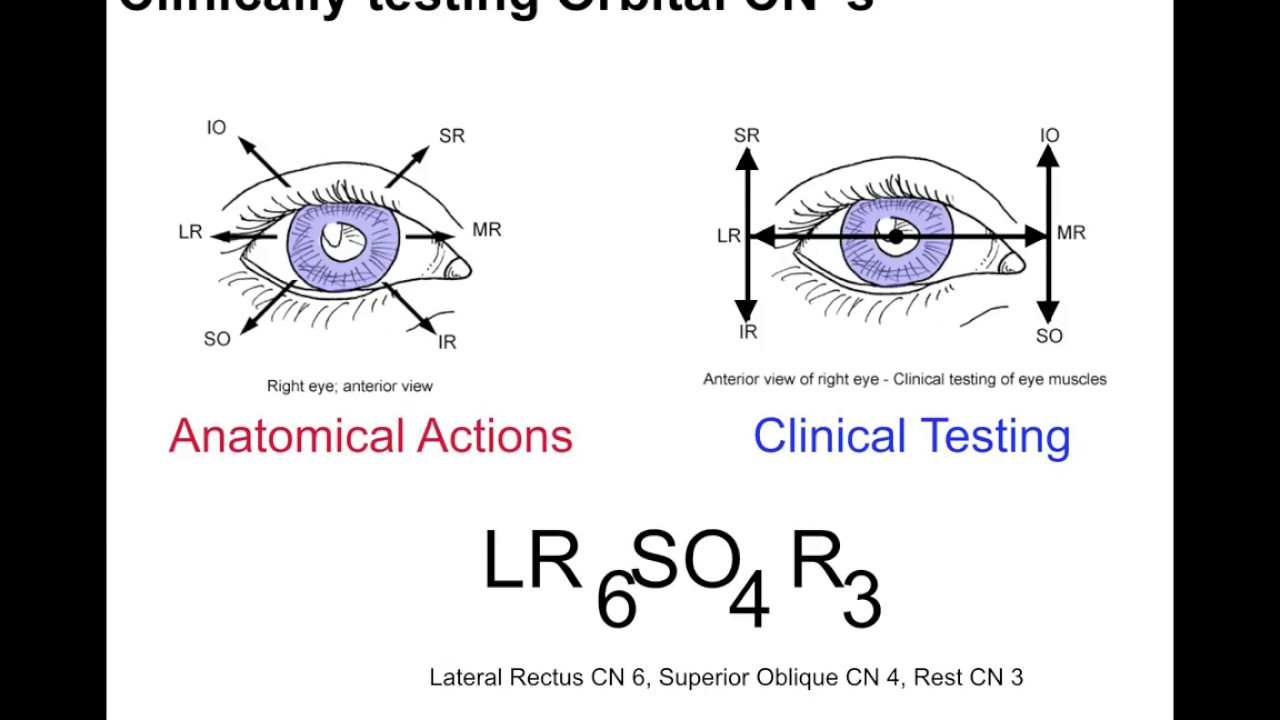
- CN abnormalities teased out by “H” test
- Visual Acuity deficits - if they can’t see, we can’t help them; can’t have DVA w/o basic acuity.
- https://locate.covd.org/ - find a neuro-optometrist.
Vestibular Assessment:
- VOMS: See above
- Head Impulse Test: not as sensitive in those with mild to moderate vestibular loss (often the case with concussion more-so than severe vestibular loss when the head impulse test is more likely to be positive).
- BPPV:
- Dix-Hallpike
- Roll Test
- Treat what you find. If nystagmus does not beat in expected direction, think central
- Exception: downbeating torsional away from ear being tested in dix-hallpike, could potentially be near common crus and can potentially be treated w/ “Quick Liberatory Rotation Maneuver”
Migraine Assessment:
- Migraines are caused by high sensitivity due to poor adaptation.
- Central stimulation builds until it hits a critical threshold which starts a migraine attack

Migraine Trigger Categories:
- Physiological:
- Hormones (menstruation, pregnancy, menopause), allergies, dehydration, hunger, sleep changes (too much or too little), exercise (too much or too little).
- Environmental:
- Odors, pain, touch, visual, sound, motion, barometric pressure changes
- Food/Medication
- Difficult to identify or prove
- Aged cheeses, salty foods, aspartame, MSG, alcohol (esp. wine), other fermented drinks, caffeine, oral contraceptives, vasodilators (nitroglygerin)
Stages of Migraine:
- Prodrome
- Sx may occur 1-2 days prior to attack
- Constipation, mood changes (euphoria, depression), food cravings, neck stiffness, increased thirst/urination, frequent yawning.
- Aura
- Nervous system Sx 20-60 minutes prior to onset of headache
- Visual phenomena, vision loss, tingling or pins and needles in arms or legs, weakness or numbness in face or laterality, difficulty speaking, hearing noises/music, uncontrollable jerking or movements.
- Attack
- 4-72 hours
- Pain on one or both sides of head, throbbing or pusling pain, sensitivity to light, sounds and sometimes touch and smell, nausea/vomiting, blurred vision, lightheadedness/fainting.
- Post-drome
- Lingering Sx following migraine. Usually lasts 24 hours
- Confusion, moodiness, dizziness, weakness, sensitivity to light and sound, mild headache w/ head in dependent position.
What does Migraine mean for Concussion Treatment?
- Much of concussion treatment is essentially graded exposure to symptom triggering stimuli
- Migraines increase the sensitivity of the brain and mark the dominant profile of limitation to recovery.
- Intermittent relief is needed to determine triggers and regulate exposure to those triggers
- Medication management may be necessary if migraines are occurring too frequently and/or patient is unable to leave to post-drome stage
Migraine Treatment:
- Start the exposure
- Will likely have initial poor ability to expose themselves to their exercises in the post-drome phase and may note a drop in exercise intensity.
- Can be discouraging and may take 1-3 days to recover to their previous levels. Visual exercises will be more difficult, higher sensitivity to dizziness and exertion; headaches may worsen.
- Take it slow after a migraine, but keep doing something.
Migraine Diagnostic Criteria:
Links to resources / articles:
Note: Much of the ocular assessment piece was gathered from a course that I attended through Upstream Rehab Institute. The information within this document was largely derived from that course.
Comments
Post a Comment