Vestibular Evaluation and Treatment
Vestibular Diagnosis and Treatment
Components of Balance
- Visual
- Somatosensory
- Vestibular
- Head motion and angular acceleration detected by the semicircular canals
- Posterior Canal
- Horizontal Canal
- Anterior Canal


- Head motion (acceleration) and head position (gravity) dependent on utricle and saccule
- Utricle: horizontal
- Saccule: vertical
- Inputs from vestibular organs, visual, proprioceptive and tactile inputs integrated in the central nervous system.
- Forebrain perceives orientation
- Spinal cord and cerebellum are responsible for postural control
- Ocular system controls eye movements
- At the base of each semicircular canal sits an ampula; within each ampula sits a cupula
- Cupula is gelatinous and has the same density as endolymph.
- The cupula is attached to hair cells which are polarized
- The cupula forms an impenetrable barrier between the ampula and the semicircular canals, so otoconia are only able to enter the semicircular canals from the end opposite the ampula.
- Eye movements are linked to cupula movements
- Crystals on cupula causes abnormal input to vestibular system and thus dizziness/nystagmus when that canal is stimulated.

Nerve Structure and Reflex
- Vestibular Reflexes
- Vestibulospinal Reflex (VSR): Descending reflex; relays information from vestibular nuclei (located in rostral medulla and caudal pons) to motor neurons that right the bodies position in space to maintain upright.
- Vestibulocolic Reflex (VCR): Righting reflex for positional stabilization of the head
- Ex: Riding on a raft and head remains upright as body moves under neck and head
- Those with neck pain and decreased motion one direction will have decreased stimulation that way and a down regulated VCR.
- Vestibulocular Reflex (VOR): Reflex to stabilize images on the retina during head movements to the opposite direction.
- Cervical Reflexes
- Cervicoocular Reflex (COR): Eye movements driven by proprioceptors in the cervical spine.
- Cervicocolic Reflex (CCR): Stretch reflex of the cervical musculature for righting of head position.
- Cervicospinal Reflex (CSR): Change in limb position driven by activity relayed from neck afferents.
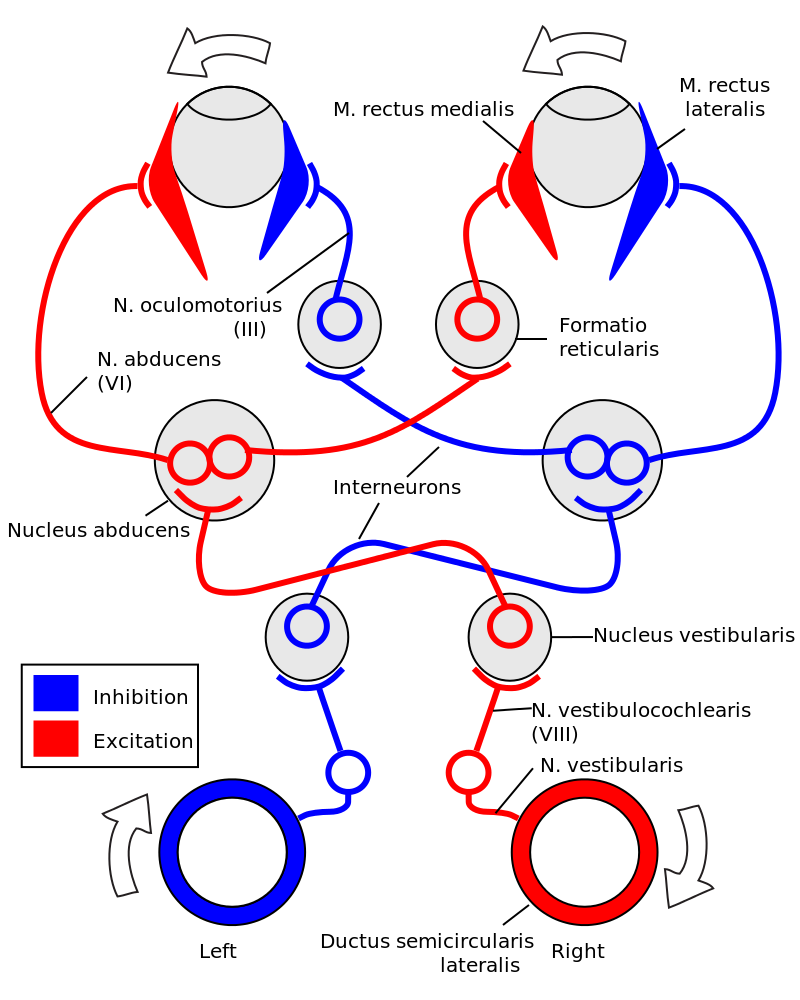
- Turning your head to the right causes right excitation and left inhibition.
- Right excitation causes stimulation of the L lateral rectus and R medial rectus (inhibition of L causes inhibition of R lateral rectus and L medial rectus) resulting eye movement opposite the direction of the head turn at a 1:1 ratio.
Nystagmus
- Corrective saccades that occur when there is a disruption in the VOR.
- The anterior and posterior canals communicate with CN III, IV and VI
- Horizontal canal only communicates with VI (purely horizontal nystagmus)
- Dizziness or vertigo?
- Dizziness: sense of imbalance or unsteadiness; dysequilibrium
- Vertigo: True sensation of spinning when the patient is not actually moving
- Vertigo with position change, especially with rolling in bed - think BPPV.
- Blood pressure (orthostatic?)
- Blood volume/dehydration
- Cancer
- Cerebellar Dysfunction
- Somatosensory dysfunction
- Neuropathy
- Vestibular Disorders
- VBI
- BPPV
- Most common form of vertigo
- Brief episodes of vertigo related to head movements
- 90% of all cases of vertigo are BPPV
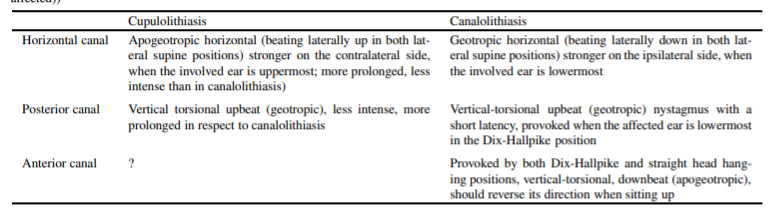
- Canalithiasis vs. Cupulolithiasis
- Canalithiasis: Otoconia (crystals) escape from the utricle and enter the semicircular canal - most commonly posterior
- Sx will fatigue with testing as otoconia settle in canal
- Cupulolithiasis: Otoconia escape from the utricle and become stuck to the cupula
- Sx will not fatigue with testing as cupula continues to be abnormally stimulated from weight of otoconia as long as patient remains in testing position.
- Idiopathic BPPV - ~50-70%
- Secondary BPPV - 7-17% (most commonly from trauma, more likely to be b/l because of the release of numerous otoconia into the endolymph)
- Vestibular Neuronitis - ~15% (also called viral neurolabyrinthitis)
- Meniere’s Disease
- True etiology is unknown but it is linked with issues in the endolymphatic system and increased fluid in the inner ear (benefit from low sodium diet and diuretics)
- Common Sx:
- Unilateral hearing loss
- Feeling of fullness in the involved ear
- Tinnitus
- Antihistamine (zyrtec or allegra) my help
- Meiniere’s and Migraines also linked.
- Post Concussion syndrome
- Common areas of concussion deficits
- Cognitive/fatigue
- Vestibular/ocular
- Physical/exertional
- Cervical
- Emotional
- Post-traumatic migraine
- Acoustic Neuroma
- Benign tumor of Schwann cells of the vestibulocochlear nerve
- If neuroma is close to vestibular portion of the nerve it can cause vertigo.
- Vestibular Migraine
- At least 5 episodes of vestibular Sx of moderate to severe intensity lasting 5 minutes to 72 hours
- Hx of migraine w/ or w/o aura
- One or more migraine features w/ at least 50% of the episodes (aura, photophobia, phonophobia, dizziness)
- Get blue light filters for computer screens, or wear amber tinted lenses to filter blue light for those with sensitivity to screens.
- Migraine is mostly a vascular problem, MTT tends to increase blood flow, gold standard for PT treatment is manual.
- Dx of exclusion
- Cervicogenic Dizziness
- Disequilibrium/swimming sensation, often associated with neck pain headaches
- Cervical ROM restrictions
- Vertebrobasilar Insufficiency (VBI)
- Be sure to rule out
- “Headache like no other”
- Double vision, ptosis of the eye, new onset of CN impairments, facial movement changes, Horner’s syndrome
- 5 D’s 3 N’s
- Dizziness, diplopia, dysarthria, dysphagia, drop attacks
- Nausea, nystagmus, numbness
- Unilateral or Bilateral vestibular lesion
- Anything that disrupts conduction along the vestibular nerve or spinal tract
- Ex: Tumor, medications virus, toxicity (heavy metals, platinum chemotherapy), CVA

Causes of Dizziness:
- Acute Vestibular Syndrome: Acute persistent continuous dizziness lasting days to weeks and usually associated with nausea, vomiting, and intolerance to head motion.
- Vestibular Neuritis
- Labyrinthitis
- Posterior Circulation Stroke
- Demyelinating Diseases
- Post-traumatic vertigo
- Triggered Episodic Vestibular Syndrome: Episodic dizziness triggered by specific and obligate actions, usually a change in head or body position w/ episodes generally lasting < 1 minute
- BPPV
- Postural Hypotension
- Perilymph Fistula
- Superior Canal Dehiscence Syndrome
- Vertebrobasilar Insufficiency (VBI)
- Central Paroxysmal Positional Vertigo: Rare, from a structural lesion (tumor, stroke, MS plaque) generally in cerebellar vermis or 4th ventricle
- Spontaneous Episodic Vestibular Syndrome: Episodic dizziness that occurs w/o a trigger that lasts minutes to hours.
- Vestibular Migraine
- Meniere’s Disease
- Posterior Circulation Transient Ischemic Attack (TIA)
- Medication side effects
- Anxiety or Panic Disorder
- Chronic Vestibular Syndrome: Dizziness that lasts weeks to months or longer.
- Anxiety or panic disorder
- Medication side effects
- Post-traumatic Vertigo
- Posterior Fossa Mass Lesions
- Cervicogenic vertigo
- Otologic Disorders
- Meniere’s disease - episodic attacks w/ sustained vertigo with fluctuating hearing loss, feelings of aural fullness and tinnitus in involved ear.
- Acute peripheral vestibular dysfunction syndromes: Sudden, unanticipated severe vertigo with a subjective sensation of rotational (room spinning) motion - commonly preceeded by a viral prodrome. Vertigo is of gradual onset and lasts for days to weeks and present at rest though it may be exacerbated w/ position changes.
- Vestibular neuritis: can potentially put pressure on cochlear portion of the nerve and cause hearing loss.
- Labyrinthitis: labyrinthine artery supplies bloodflow to the vestibular aparatus and conchlea so if affected can result in hearing loss and tinnitus.
- Superior Canal Dehiscence Syndrome: attacks of vertigo and oscillopsia as well as potentially nystagmus that is often exacerbated by loud sounds, valsalva maneuver, or pressure changes of the external auditory canal (tragal pressure)
- Perilymph Fistula: Vertigo and nystagmus related to pressure changes (tragal pressure)
- Neurologic Disorders
- Nystagmus findings that likely indicate a non-peripheral cause of nystagmus:
- Pure down-beating with dix-hallpike
- Direction changing nystagmus that occurs w/o change in head position.
- Direction switching nystagmus (right beating with right gaze, left beating with left gaze).
- Resting nystagmus (could also be vestibular neuritis)
- Other eye movements not indicative of BPPV:
- Intenuclear opthalmoplagia: affected eye fails to adduct during conjugate gaze to opposite side: R eye fails to adduct when looking L
- Lesion of the R medial longitudinal fasciculus.
- Medications that may potentially cause dizziness/vertigo
- Mysoline
- Carbamazepine
- Phenytoin
- Sedatives
- Anti-hypertensives
- Cardiovascular medications
Objective Exam:
- Cervical Spine
- AROM: Is there reproduction of dizziness with sustained end range cervical ROM.
- Upper Cervical Instability (UCI) Testing:
- Sharp’s Purser: (+) for UCI w/ alleviation of Sx or clunk as C1 reduces on C2
- C2 kick: Alar Ligament: feel for a subtle kick into opposite hand with side bend through upper cervical spine. Lack of kick is considered positive for contralateral alar ligament.
- Transverse Ligament: Supine, support occiput and C1 and provide an anterior glide as gravity pushes caudal segments posteriorly.
- Spurling Test: Cervical Radiculopathy
- ULTT
- DTR: Hyper = UMN; Hypo = LMN
- Hoffman: UMN
- Head Shake Test: Rapid head shaking by clinical at a rate of 1-2 Hz, may see nystagmus upon ceasing w/ peripheral vestibular dysfunction (tested with frenzel’s)
- Head Impulse Test (Head Thrust Test): Patient focuses eyes on the tip of therapists nose; rotate head side to side, quick jerk back to middle. Look for corrective saccade to indicate peripheral vestibular dysfunction. (positive w/ BPPV and/or vestibular hypofunction)
- Saccade will occur toward the involved ear
- Test can also be performed w/ a lateral thrust (as opposed to a rotational thrust) in order to bias the utricle which senses lateral movements
- Cranial Nerve Testing: Involvements in more than just vestibulo-ocular could indicate brainstem lesion.
- Cervical Body Rotation Test: Test for reproduction of dizziness with head stable rotating body. Eyes remain fixed with no head movement so vestibular and visual systems are not being tested.
- MMT: Myotomes, cervical spine, DNF
- Grip Strength: Unilateral nerve root irritation
- Balance
- Rhomberg:
- Difficulty w/ firm EO indicates need for upregulation of all systems as simply narrowing BOS and eliminating use of UE causes poor balance.
- Difficulty w/ firm EC indicates patient requires good visual input as their vestibular and somatosensory systems are unable to compensate for the decreased visual input (make sure they have night lights in their house)
- Difficulty w/ foam EO indicates patient requires good somatosensory input as their visual and vestibular systems are unable to compensate for the less stable surface.
- Difficulty with EC Foam, but nothing else indicates need to upregulate vestibular system as it is unable to compensate when other inputs are removed/decreased.
- Single Leg Stance
- EO firm/foam
- EC firm/foam
- Tested hands on hips.
- **Rhomberg may have a ceiling effect in higher functioning individuals so you may be able to tease out more with SLS.
- Motor Planning
- TUG:
- Initiation of movement (primary motor cortex and premotor cortex)
- Coordination with walking/turning (cerebellum)
- Change in position (orthostatic)
- Dysmetria:
- Nose to finger
- Heel to shin
- Assessing for cerebellar dysfunction
- Dysdiadochokinesia:
- Rapid alternating hand movements
- Assessing for cerebellar dysfunction
- Babinski: Assessing for UMN lesion
- DGI:
- Walking: Assess overall quality and speed of gait
- Walking with Head Turns: Assesses vestibular system
- Horizontal
- Vertical
- Walking with change in gait speed
- Gait w/ pivot and turn
- Step over obstacle
- Weave through obstacles
- Stairs
- FGA: Same as DGI, removes weaving through cones; adds a time component to gait and adds backward walking, walking with eyes closed and heel-to-toe walking to account for ceiling effect with DGI.
- Use DGI with lower functioning and FGA w/ higher functioning.
- Oculomotor Testing
- Dynamic Visual Acuity
- Tested at 2 Hz (2 cycles per second) in the literature
- Pretty fast
- Patient reads the lowest line that they are able to with both eyes at a distance of 20’ from chart
- Therapist stands behind patient, grips head and rotates side to side at a rate of 120 bpm
- Positive is a loss of 3 lines or more in the literature (2 lines or more at the course with patient self selecting a decently fast speed)
- Smooth Pursuits:
- CN III, IV, VI
- VOR assessment: Assess at 180 bpm horizontal and vertical; impaired VOR will cause potentially cause dizziness and patient will be unable to keep image clear as the image is not focused on the retina.
- Saccades: Overshooting indicates potential cerebellar; assess horizontal and vertical
- Convergence: > 6cm is considered abnormal
- Bring pen to nose (or tongue depressor w/ letter of size 14 font) have patient let you know when it becomes double (not blurry)
- BPPV
- Seated Body Rotation Test: r/o cervicogenic dizziness
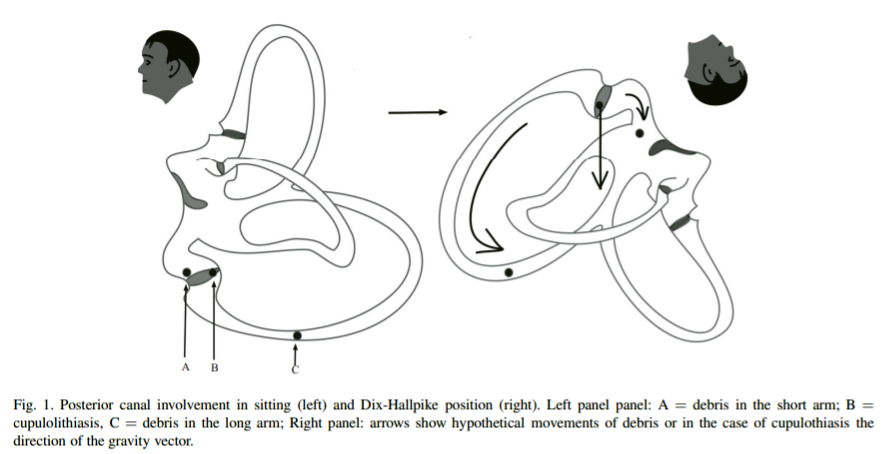
- Posterior Canal
- Dix-Hallpike: Test the ear that you suspect first, if symptomatic, begin repositioning with tht modified-epley maneuver, if other side is more symptomatic, reverse your repositioning maneuver as they will normally be less symptomatic in position 2 than position 1.
- Be sure to get head into enough extension (20 degrees).
- When you go from position 1 to position 2, there is likely minimal movement on the otoconia.
- With step 3, tuck the chin toward their shoulder and have head 45 degrees from the sagittal plane in order to dump otoconia. If the head comes into extension you may just dump the crystals right back from where they came and if you do not get the head to 45 degrees from the sagittal plane and the ears end up on top of eachother you risk dumping it in the horizontal canal.
- If you dump it in the horizontal canal (lateral nystagmus and potential vomiting/nausea) perform a Gufoni Maneuver - maintain them in this position for 2 minutes then turn the head 45 degrees downward and hold for 2 minutes and slowly return to sitting position.
- Sidelying Test
- Turn head 45 degrees away from side that you are testing and lie patient onto side that you are testing
- Ex: testing L ear, turn head R, then lie patient on L side
- To reposition, sit patient up, turn them so they are facing the opposite direction on the table and turn their head to the uninvolved side
- Ex: Repositioning L ear, turn head L and lie on R side (R ear down) - position 2
- Wait 30” after Sx fatigue and turn their head into position 3 of modified epley
- 30” after Sx fatigue sit them up.
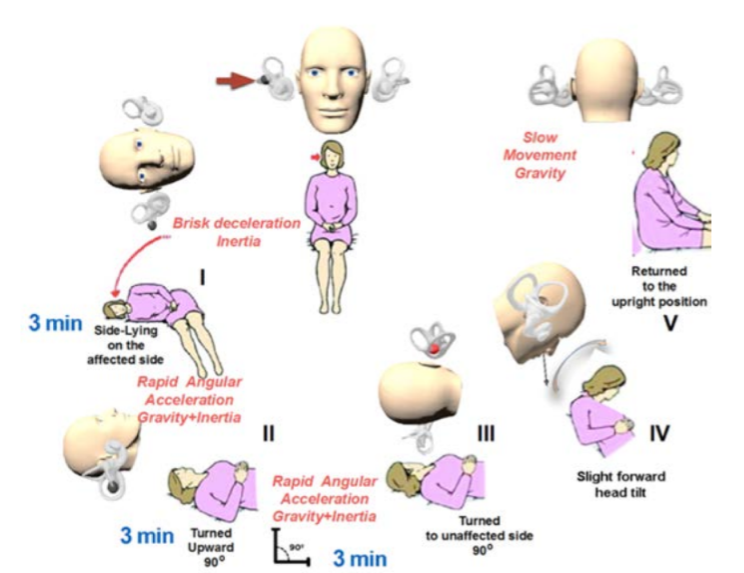
- Semont Maneuver
- Use with cupulolithiasis (non-fatiguing nystagmus with Dix-hallpike)
- Patient is seated, turn head 45 degrees away from symptomatic side and quickly lie on involved side.
- Can give the mastoid a little hit with a cupped hand to help dislodge.
- After 1-2 minutes, QUICKLY sit patient up flip them to their other side turning their head into modified epley position 3 (45 degrees from the sagittal plane with chin tucked)
- Horizontal Canal
- Assess with the roll test
- Flex head to 30 degrees, lie supine, rotate head to the side maintaining 30 degrees flexion, be sure to get ear on top of ear.
- Look for pure lateral nystagmus
- Assess other side
- Treat with Gufoni maneuver (for canalithiasis)
- Lie patient on less symptomatic side (originally studied for 2 minutes, probably don’t have to have them there that long)
- After 2 minutes turn head 45 degrees toward the ground and hold for 2 minutes
- Sit patient up
- Casani maneuver is the same thing except you lay the patient on their more symptomatic side
- Apiani is unaffected ear but turn head up?
- Can also treat with the Kurtzer Hybrid Maneuver
- After performing the roll test, lie the patient on the subjectively weaker side with the head flexed to 30 degrees.
- Then turn the head 90 degrees so their nose is facing down, maintain the head in 30 degrees of flexion
- Turn the head back up to the starting position maintaining the neck in 30 degrees of flexion and rotate their lower torso to the opposite side and perform the same maneuver (head turned down w/ nose facing the ground w/ head in 30 degrees of flexion) to the opposite side.
- This is technically the end of the KHM, but you can retest by having the patient turn their head to the side so that their head is in neutral (ear on top of ear)
- Each position is held for 1 minute after the resolution of Sx/nystagmus.
- Flow toward the ampulla (ampullopetal) is excitatory for the horizontal canal meaning that in R side lying the eyes will move left and then have a corrective saccade to the right. When lying on R side testing the horizontal canal, you should see nystagmus toward the down ear, or geotropic.
- If the cause is cupulolithiasis, lying on the R side will cause an ampullofugal flow. Ampullofugal flow is inhibitory for the horizontal canal and thus you will see eye movement to the right, and a corrective saccade to the left, or apogeotropic.
- Ewald’s Second Law: The response to an excitatory stimulus is always stronger than the response to an inhibitory stimulus which is why the nystagmus beats more toward the involved ear
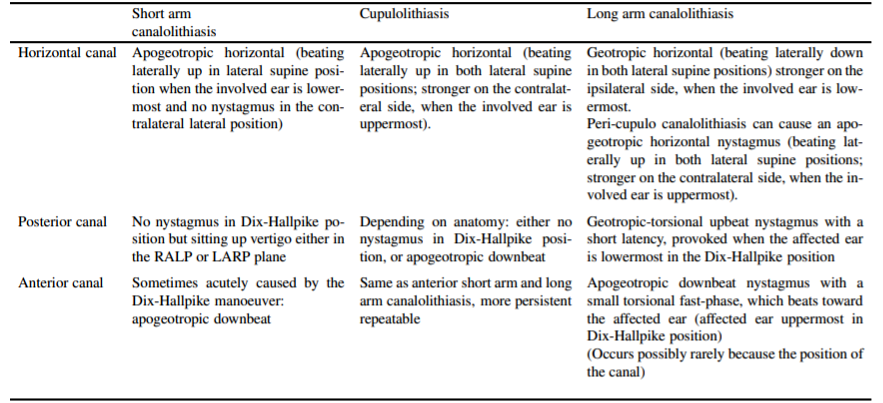
- Horizontal Canal Cupulolithiasis
- Will see apogeotropic nystagmus w/ roll test bilaterally
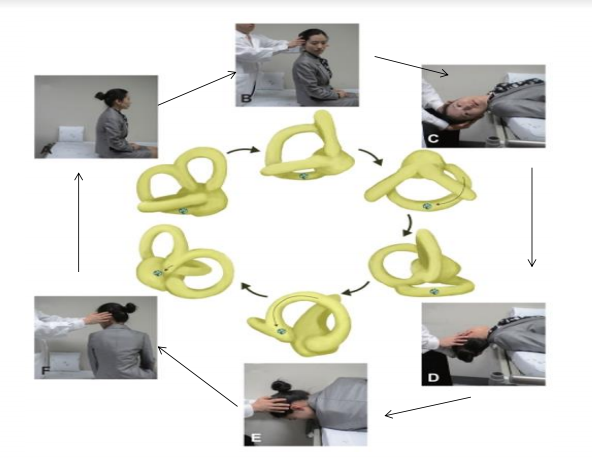
- Repositioning
- Quickly lie patient on less symptomatic side (which would be their affected side) (3 min)
- Quickly turn head 90 degrees toward the ceiling (3 min)
- Quickly turn head another 90 degrees so patient is lying on initially more symptomatic side (3 min)
- Tilt the head slightly forward (encourages particles to move toward the utricle and not into the lumen of the HC when patient returns to sitting) - 15-30”
- Return patient to sitting (at this point hopefully the otoconia fall back into the utricle)
- Likely do not have to hold for the full 3 minutes as described

- Anterior Canal
- Assess with Deep Head Hang Test
- (+) is pure upbeating nystagmus
- Reposition with the Yocovino Maneuver
- Deep Head Hang → QUICKLY move into 30 degrees of cervical flexion (hold 2’) → sit patient up
- Can also reposition with Reverse Semont
- Start with faceplant into position 3 of epley then quickly turn patient to other side face up then return to sitting.
- May also see downbeating nystagmus w/ torsion toward the dependent ear while testing dix-hallpike w/ anterior canal involvement, if you do, assess deep head hang.
- Caution** pure downbeating nystagmus can indicate brainstem or cerebellar lesion
- Short Arm BPPV
- If patient gets symptoms with return from hallpike, but not with the positioning think short arm.
- Ex: Sx w/ sitting up from R hallpike but not when sitting up from L hallpike
- Reposition with quick repetitive hallpikes
- Lay back into hallpike, sit up quickly, repeat 5x.
- 3 Domains
- Vision
- Smooth Pursuits
- Saccades
- VOR
- Convergence
- Space in motion sensitivity/VOR Cx
- Progression of visual Exercises
- Blank background objects stationary → complex background objects stationary → blank background objects moving → complex background objects moving
- Work in head movements to make more complex
- Proprioception
- Ways to progress
- Decrease base of support, decrease stability of surface
- Feet together → tandem → single leg
- Firm → Foam → Bosu
- Can work on bouncing, marching etc. on different surfaces.
- Vestibular
- Change in velocity and direction of head movement
- Increase speed
- Alter planes of motion (sagittal, transverse, frontal, diagonals, complex)
- Vestibular Exercises
- VOR x 1: Object stable, move head
- Lateral movements target Horizontal Canal
- Vertical head movements target Anterior Canal
- Oblique head movements target Posterior Canal
- VOR x 2: Move object and head
- Make sure to stay w/in field of vision
- Can work all planes
- 2 Target VOR: Eyes and head on one target -> eyes move to other target -> head follows
- Make sure to stay w/in field of vision
- Can work all planes
- Imaginary Targets:
- Keep eyes on target -> close eyes -> rotate head trying to keep gaze on target -> open
- Goal is to have eyes fixed on target when they open.
- Translational VOR:
- Same as VOR but targets utricle and saccule more
- Lateral movements: utricle (lateral, not tilting movements)
- Vertical movements: saccule (can do by bouncing on a PB or bed)
- Other exercise ideas:
- Stand on unsteady surface, maintain gaze on a target, squat
- Stand on unsteady surface, bow and look up, can also work on diagonal bowing
- Stand on unsteady surface and do bouncing to work on balance and maintaining gaze (can also do on PB)
- Walking w/ head turns
- Walking VOR
- Reading a magazine on the treadmill
- Walking and grabbing ball from therapist behind them that places the ball in different areas so they have to turn and find it while walking
- Sit to stands w/ feet on unsteady surface, with head movements
Medications:
- Benzodiazepines: Clonazepam, diazepam - reduce the subjective sensation of spinning and can also interfere with central compensation
- Antihistamines: meclizine, diphenhydramine - suppress the central emetic center to help relieve nausea and vomiting.
- Meclizine helps control: nausea, vomiting and the sensation of spinning - useful in the acute phase, but will not help with feelings of unsteadiness, or with VOR deficits.
- Other medications to avoid before eval and for Sx if cause is BPPV
- Promethazine
- Ondansetron - serotonin 5HT3 antagonist
- Anticholinergic drugs - scopolamine (blocks ACh)6u
- Embedded Saccades: Once a patient learns that their VOR is impaired, they can begin to practice maintaining their gaze on a target and as they feel their head turning, they will be proactive and create a saccade as their head is moving as opposed to after (such as seen with head impulse test).
- Not the most energy efficient because it requires some conscious effort but it will improve ability to see during dynamic activity.
Comments
Post a Comment